History
A 12 year old bay American Quarter Horse mare was noted by her owner to have behavioral changes over the past year. The normally placid mare was beginning to show aggressive behavior toward other mares. The owner indicated that the mare had never had a foal previously and had not been bred this year.
Physical Examination
The mare was determined to be in good condition with a body condition score of 6. Examination of the external genitalia revealed that the vulva was in a normal vertical position, with good muscular tone and approximately 75 % of the vulva was below the pelvic brim.
Behavioral Evaluation
The mare was allowed to approach a second mare that was known to be in heat.
The affected mare teased the mare in heat as if she were a stallion (see video).
The mare in heat responded to the affected mare by posturing to urinate, etc.
Ultrasound Examination
A transrectal ultrasound examination was subsequently performed. The left ovary was determined to be enlarged (approximately 10 cm in diameter) and contained numerous cystic pockets (Figure 1). The contralateral right ovary was small and exhibited limited follicular development (Figure 2). Examination of the uterus indicated that the mare was not pregnant.
A 12 year old bay American Quarter Horse mare was noted by her owner to have behavioral changes over the past year. The normally placid mare was beginning to show aggressive behavior toward other mares. The owner indicated that the mare had never had a foal previously and had not been bred this year.
Physical Examination
The mare was determined to be in good condition with a body condition score of 6. Examination of the external genitalia revealed that the vulva was in a normal vertical position, with good muscular tone and approximately 75 % of the vulva was below the pelvic brim.
Behavioral Evaluation
The mare was allowed to approach a second mare that was known to be in heat.
The affected mare teased the mare in heat as if she were a stallion (see video).
The mare in heat responded to the affected mare by posturing to urinate, etc.
Ultrasound Examination
A transrectal ultrasound examination was subsequently performed. The left ovary was determined to be enlarged (approximately 10 cm in diameter) and contained numerous cystic pockets (Figure 1). The contralateral right ovary was small and exhibited limited follicular development (Figure 2). Examination of the uterus indicated that the mare was not pregnant.


Figure 1. Ultrasound image of the enlarged left ovary
(bracket). Note the multi-cystic appearance of the ovary
(arrow).
Figure 2. Ultrasound image of the smaller right ovary
(bracket). Note the general lack of follicular activity.
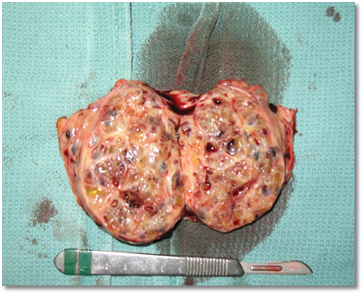
Figure 3. Photograph of the enlarged left ovary after
surgical removal.
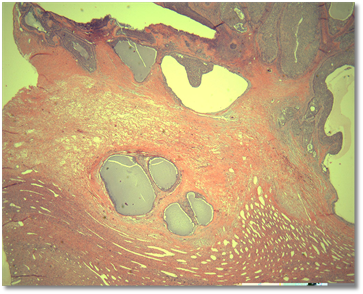
Figure 4. Histopathology of the affected ovary.
~~~~~
The goal of this report is to provide veterinarians and horse owners with an educational opportunity based on an actual
clinical case presented to the Equine Reproduction Laboratory at Colorado State University. Publication of the report is
sponsored by Animal Reproduction Systems, Chino, CA.
For more information on equipment and supplies available at ARS, please visit our website at www.arssales.com or call us
at (800) 300-5143
Equipment described in this case report available at Animal Reproduction Systems includes:
Equine Reproduction Case Files
|
August 2013
|
Issue No. 3
|
Treatment
Surgical removal of the affected ovary was recommended. The enlarged left ovary
was removed (Figure 3) and a biopsy was submitted for histopathologic analysis,
which confirmed the diagnosis of a granulosa-theca cell tumor (Figure 4).
Hormone
|
Value in Clinical Case
|
Normal Range
|
Inhibin
|
2.69 ng/ml
|
0.1 to 0.7 ng/ml
|
Testosterone
|
144.3 pg/ml
|
20 to 45 pg/ml
|
Progesterone
|
0.2 ng/ml
|
< 1.0 in estrus or anestrus
? 1.0 in diestrus
|
Anti-Müllerian Hormone
|
Not determined
|
< 1.0 ng/ml
|
Granulosa Cell Tumor in a Mare
By Patrick M. McCue, DVM, Ph.D.,
Diplomate American College of Theriogenologists
By Patrick M. McCue, DVM, Ph.D.,
Diplomate American College of Theriogenologists
Differential Diagnosis
Based on the history provided by the owner and the initial ultrasound examination, two lists of potential clinical diagnoses were formulated.
Differential Diagnoses for an Enlarged Ovary:
-Ovarian tumor
-Granulosa cell tumor or granulosa-theca cell tumor
-Cystadenoma
-Teratoma
-Hemorrhagic Anovulatory Follicle
-Ovarian Hematoma
-Pregnancy
Differential Diagnoses for Aggressive or Stallion-like Behavior:
-Granulosa-theca cell tumor
-Pregnancy
-Anabolic steroid administration
-Developmental abnormality
-Chromosomal abnormality
Based on the history provided by the owner and the initial ultrasound examination, two lists of potential clinical diagnoses were formulated.
Differential Diagnoses for an Enlarged Ovary:
-Ovarian tumor
-Granulosa cell tumor or granulosa-theca cell tumor
-Cystadenoma
-Teratoma
-Hemorrhagic Anovulatory Follicle
-Ovarian Hematoma
-Pregnancy
Differential Diagnoses for Aggressive or Stallion-like Behavior:
-Granulosa-theca cell tumor
-Pregnancy
-Anabolic steroid administration
-Developmental abnormality
-Chromosomal abnormality

Ovarian tumors are typically unilateral. The granulosa or granulosa-theca cell tumor is a hormone producing neoplasia that can suppress follicular development in the contralateral ovary. Inhibin and androgens produced by the tumor suppresses production and secretion of follicle stimulating hormone (FSH) from the anterior pituitary. Follicular development decreases in the otherwise normal contralateral ovary in the absence of FSH support. Other ovarian tumors such as the cystadenoma and teratoma are not hormonally active and therefore do not have a suppressive effect on the contralateral ovary.
Hemorrhagic events can also cause unilateral enlargement of the ovary. Hemorrhage may occur into a dominant follicle prior to ovulation resulting in a hemorrhagic anovulatory follicle. Initially the blood does not clot within the follicle due to the presence of a heparin-like molecule within equine follicular fluid. Eventually however the blood clots and granulosa and theca cells invade into the blood clot and luteinize, resulting in an increase in blood progesterone levels.
Excessive hemorrhage into the collapsed follicle after ovulation is an uncommon occurrence and results in a structure referred to as an ovarian hematoma. This will also result in formation of a luteal structure and production of progesterone.
Pregnant mares will usually have bilaterally enlarged ovaries in the second to fourth month of pregnancy due to the formation of secondary corpora lutea. Secondary CLs develop in response to production of equine chorionic gonadotropin (eCG) by endometrial cups which invade into the maternal endometrium beginning at approximately 35 days of gestation. In addition, pregnant mares can exhibit signs of masculinized behavior during the middle of gestation due to production of testosterone from the fetal gonads. Concentration of testosterone in maternal blood peaks at around 200 days of gestation.
Administration of anabolic steroids can also cause aggressive behavior, but is not associated with ovarian enlargement. In fact, anabolic steroid administration will decrease secretion of FSH and result in suppression of follicular activity and inactive ovaries.
Occasionally a mare will present for aggressive or stallion-like behavior and examination will reveal that the horse has the external phenotype of a mare, but the genetic or chromosomal constitution of a stallion (i.e. an XY karyotype) and cryptorchid testes. The term for such a horse is a male pseudohermaphrodite.
Endocrine Testing
In order to confirm the clinical diagnosis and rule out other potential causes of the behavioral and ovarian changes noted, a blood sample was collected and submitted for hormone analysis (Table 1). Inhibin is a hormone produced by granulosa cells of the ovarian follicle. Inhibin levels in a normal mare increase during estrus and reach peak levels near the day of ovulation. Concentrations then decline to baseline during diestrus. The concentration of inhibin in this mare was markedly elevated above the normal range in cycling mares.
Testosterone is produced by theca cells of developing follicles and the pattern of testosterone levels during the estrous is similar to the pattern observed with estradiol. Concentrations increase during estrus and peak a day or two prior to ovulation and then decrease to low levels during diestrus. The concentration of testosterone in this mare was also significantly above the normal range of cycling mares and was likely the cause of the abnormal behavior.
Progesterone levels in normal mares increase after ovulation and are at basal levels when a mare is in estrus (heat) or when the mare is not cycling (i.e. winter anestrus). Progesterone levels may be increased in mares with transient ovarian abnormalities such as luteinized anovulatory follicles or luteinized ovarian hematomas. In contrast, progesterone is not produced by ovarian tumors. The progesterone level in this mare was at baseline level indicating a lack of luteal tissue.
Anti-Müllerian hormone (AMH) is produced by granulosa cells and has been reported to be elevated in most mares with granulosa cell tumors. Blood from this mare was not evaluated for levels of AMH.
The hormone profile in this mare was supportive of a diagnosis of a granulosa-theca cell tumor.
Table 1. Hormone profile from the mare with unilateral ovarian enlargement and aggressive behavior.
Hemorrhagic events can also cause unilateral enlargement of the ovary. Hemorrhage may occur into a dominant follicle prior to ovulation resulting in a hemorrhagic anovulatory follicle. Initially the blood does not clot within the follicle due to the presence of a heparin-like molecule within equine follicular fluid. Eventually however the blood clots and granulosa and theca cells invade into the blood clot and luteinize, resulting in an increase in blood progesterone levels.
Excessive hemorrhage into the collapsed follicle after ovulation is an uncommon occurrence and results in a structure referred to as an ovarian hematoma. This will also result in formation of a luteal structure and production of progesterone.
Pregnant mares will usually have bilaterally enlarged ovaries in the second to fourth month of pregnancy due to the formation of secondary corpora lutea. Secondary CLs develop in response to production of equine chorionic gonadotropin (eCG) by endometrial cups which invade into the maternal endometrium beginning at approximately 35 days of gestation. In addition, pregnant mares can exhibit signs of masculinized behavior during the middle of gestation due to production of testosterone from the fetal gonads. Concentration of testosterone in maternal blood peaks at around 200 days of gestation.
Administration of anabolic steroids can also cause aggressive behavior, but is not associated with ovarian enlargement. In fact, anabolic steroid administration will decrease secretion of FSH and result in suppression of follicular activity and inactive ovaries.
Occasionally a mare will present for aggressive or stallion-like behavior and examination will reveal that the horse has the external phenotype of a mare, but the genetic or chromosomal constitution of a stallion (i.e. an XY karyotype) and cryptorchid testes. The term for such a horse is a male pseudohermaphrodite.
Endocrine Testing
In order to confirm the clinical diagnosis and rule out other potential causes of the behavioral and ovarian changes noted, a blood sample was collected and submitted for hormone analysis (Table 1). Inhibin is a hormone produced by granulosa cells of the ovarian follicle. Inhibin levels in a normal mare increase during estrus and reach peak levels near the day of ovulation. Concentrations then decline to baseline during diestrus. The concentration of inhibin in this mare was markedly elevated above the normal range in cycling mares.
Testosterone is produced by theca cells of developing follicles and the pattern of testosterone levels during the estrous is similar to the pattern observed with estradiol. Concentrations increase during estrus and peak a day or two prior to ovulation and then decrease to low levels during diestrus. The concentration of testosterone in this mare was also significantly above the normal range of cycling mares and was likely the cause of the abnormal behavior.
Progesterone levels in normal mares increase after ovulation and are at basal levels when a mare is in estrus (heat) or when the mare is not cycling (i.e. winter anestrus). Progesterone levels may be increased in mares with transient ovarian abnormalities such as luteinized anovulatory follicles or luteinized ovarian hematomas. In contrast, progesterone is not produced by ovarian tumors. The progesterone level in this mare was at baseline level indicating a lack of luteal tissue.
Anti-Müllerian hormone (AMH) is produced by granulosa cells and has been reported to be elevated in most mares with granulosa cell tumors. Blood from this mare was not evaluated for levels of AMH.
The hormone profile in this mare was supportive of a diagnosis of a granulosa-theca cell tumor.
Table 1. Hormone profile from the mare with unilateral ovarian enlargement and aggressive behavior.
Take home message(s):
1. The mare in this case report presented with classic signs of an ovarian tumor and specifically a granulosa-theca cell tumor. It would have been possible to make a correct diagnosis just based on history and transrectal palpation.
2. However, additional diagnostic tests, including ultrasonography and hormone analyses, were performed to support the clinical diagnosis. A combination of elevated inhibin and elevated testosterone provide strong supportive evidence of the presence of a granulosa-theca cell tumor.
3. It is recommended that one should not be in a rush to remove an ovary unless the diagnosis is clear and unequivocal. One can always recheck the mare in 1 to 2 weeks if unsure. The most common error is the misdiagnosis of a hemorrhagic anovulatory follicle with echogenic fibrin strands crisscrossing the follicular lumen as a granulosa cell tumor. A hemorrhagic anovulatory follicle will not have an elevation in blood levels of inhibin, testosterone or AMH and will eventually have an elevation in progesterone.
4. The prognosis for return to normal behavior for this mare is excellent. The pre-surgery elevated testosterone levels which were the cause for her aggressive behavior will decrease to normal values within 24 hours after surgical removal of the affected ovary. In the absence of elevated testosterone, her demeanor should revert back to her former behavior within days or weeks.
5. Normal ovarian function should return to the remaining right ovary within an average of 6 months after surgery. If this were a broodmare, it would be anticipated that she should cycle normally (i.e. every 21 days) off the single ovary and would have a similar prognosis for fertility and ability to carry a foal to term as she had prior to the surgery.
1. The mare in this case report presented with classic signs of an ovarian tumor and specifically a granulosa-theca cell tumor. It would have been possible to make a correct diagnosis just based on history and transrectal palpation.
2. However, additional diagnostic tests, including ultrasonography and hormone analyses, were performed to support the clinical diagnosis. A combination of elevated inhibin and elevated testosterone provide strong supportive evidence of the presence of a granulosa-theca cell tumor.
3. It is recommended that one should not be in a rush to remove an ovary unless the diagnosis is clear and unequivocal. One can always recheck the mare in 1 to 2 weeks if unsure. The most common error is the misdiagnosis of a hemorrhagic anovulatory follicle with echogenic fibrin strands crisscrossing the follicular lumen as a granulosa cell tumor. A hemorrhagic anovulatory follicle will not have an elevation in blood levels of inhibin, testosterone or AMH and will eventually have an elevation in progesterone.
4. The prognosis for return to normal behavior for this mare is excellent. The pre-surgery elevated testosterone levels which were the cause for her aggressive behavior will decrease to normal values within 24 hours after surgical removal of the affected ovary. In the absence of elevated testosterone, her demeanor should revert back to her former behavior within days or weeks.
5. Normal ovarian function should return to the remaining right ovary within an average of 6 months after surgery. If this were a broodmare, it would be anticipated that she should cycle normally (i.e. every 21 days) off the single ovary and would have a similar prognosis for fertility and ability to carry a foal to term as she had prior to the surgery.